E-Case report
Disc herniation & bilateral foraminal stenosis
L4/5 MIS TLIF in ASC outpatient procedureAli M. Maziad, MD PhD

Pre OP

Clinical Case – Disc herniation & Bilateral foraminal stenosis
L4/5 MIS TLIF in ASC* outpatient procedure
Ali M. Maziad, MD PhD
Orthopedic Spine Surgeon
Maziad Spine Institute
Miami, FL, USA


* Ambulatory Surgical Center


Patient Information:
A 52-year-old female house-keeper reported severe lower back pain (LBP) as well as left lower extremity radiculopathy following a slip down the stairs.
Patient tried conservative measures including physical therapy medications and injections with limited relief.
- Height: 61.0 in/1.55 m
- Weight: 210 lbs/95 kg
- BMI: 38
On review of the MRI scan, an incidental finding of a large uterine fibroid was noted. After clearance from the gynecologist for surgery, and given her unique abdominal anatomy, surgical approaches to the spine such as ALIF or LLIF were considered contraindicated given the high risk involved.
Minimally invasive TLIF was considered more suitable for the patient given the high BMI and potential for excessive bleeding from fibroid compression on inferior vena cava.
Diagnoses:
- Decreased disc height at L4-5 level.
- L4/5 disc herniation causing central as well as bilateral foraminal stenosis, more on the left side.
- Radiculopathy left side.
- Patient was noted to have a very large fibroid on the MRI scan which was an incidental finding.


Pre OP radiographs, frontal and sagittal views




Pre OP MRI and radiograph sagittal view

Pre OP MRI scan, sagittal and axial views, showed a L4/5 disc herniation causing central as well as bilateral foraminal stenosis, more on the left side.
Patient was noted to have a very large fibroid.




Intra OP
OR-strategy:
Thoraco-Lumbar Interfascial Plane (TLIP) block, injection of local anesthetics, in level L3 – L4.
L4/5 minimally invasive TLIF – left, to be performed as an outpatient procedure in the ASC.
Planning to use the Neo Cage System ™ & Neo Pedicle Screw System™ for fusing the segment L4/5.
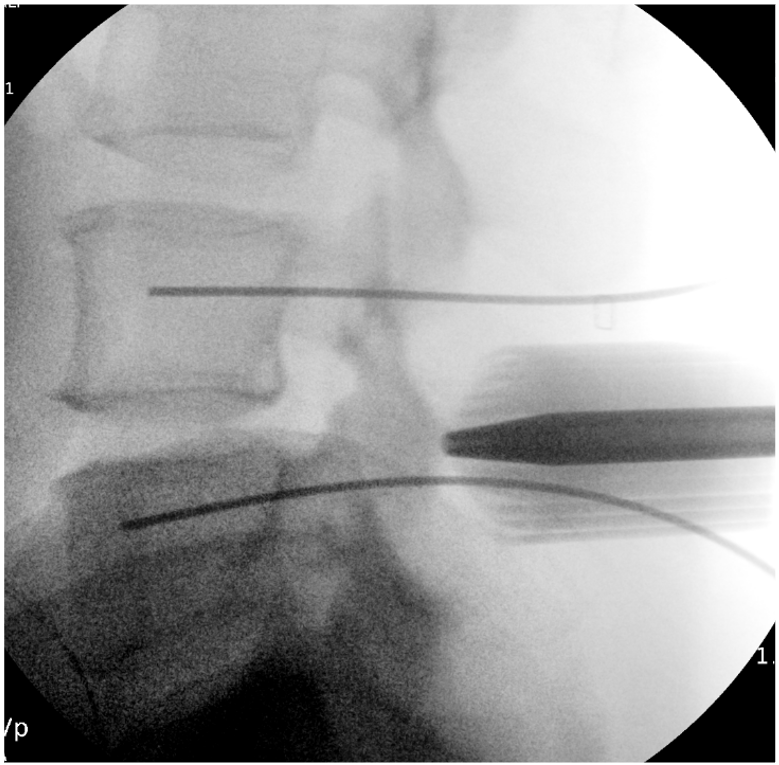
Intra OP radiograhs for the planning of the surgical access.


L5 & L4 - Access and placing the K-wires.





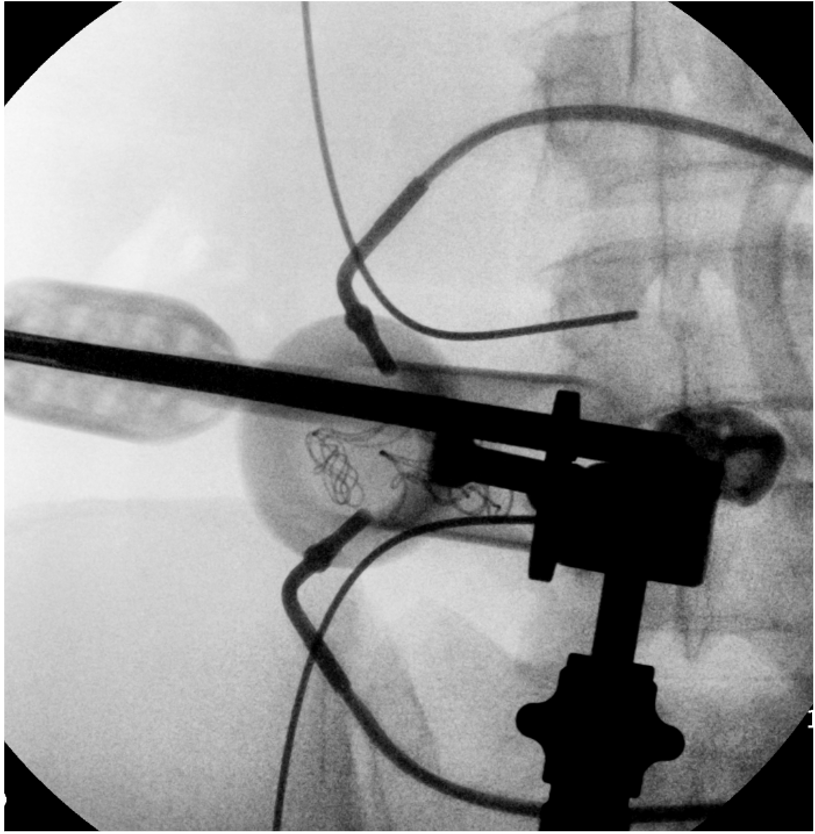
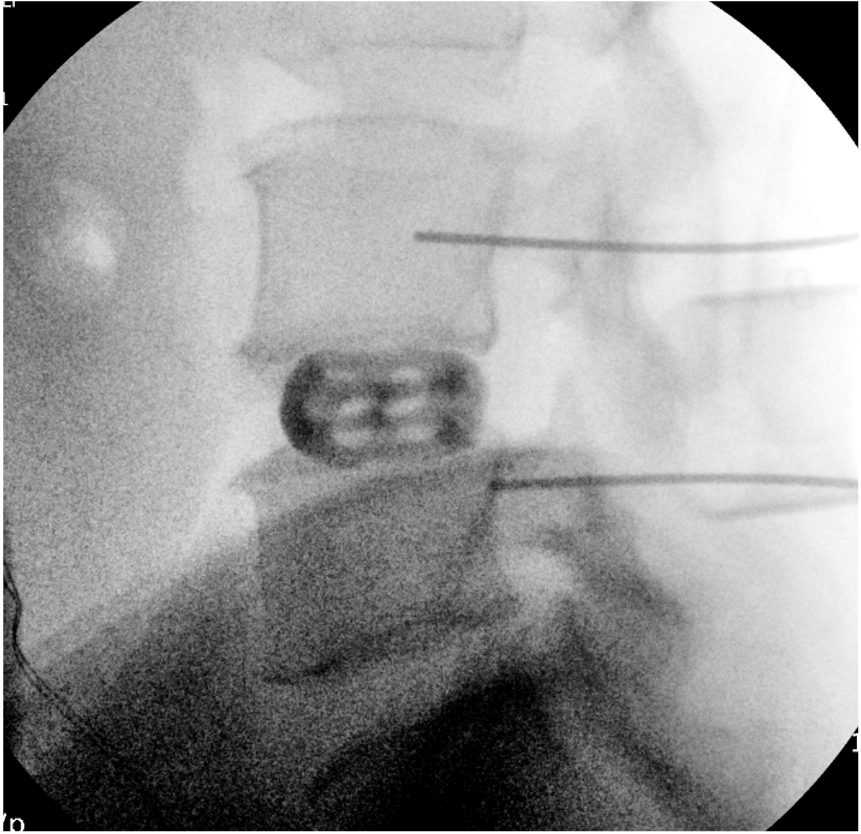
Disc space preparation and placement of Neo Cage anatomical/straight 26mm, 11mm, 0° from the left side







Inserting 4 pedicle screws,
Neo Pedicle Screw System™
L4: 2 x Ø6.0x45 mm
L5: 2 x Ø6.0x45 mm
2 x titanium rods, straight 40 mm, were placed.






Radiographs, frontal and sagittal views


Total time of surgery: 2 hours and 30 minutes
Estimated blood loss: 50 cc.
Patient had relatively excessive bleeding after facetectomy which would be attributed to the large fibroid and compression of inferior vena cava and engorgement of the epidural veins.
The minimally invasive approach was ideal for her to reduce operative time and blood loss.


Pre OP and Post OP situation
Post OP
Post OP radiographs, frontal and sagittal views.
Patient was discharged from the clinic 2 hours after surgery.
She had complete resolution of her lower extremity radiculopathy and significant improvement in her lower back pain 1 week after surgery.

Radiographs after the final fixation of the posterior construction, and removal of the instrumentation
Follow up
Radiographs at 2 months Follow Up, frontal and sagittal views

Follow up
Radiographs at 3 months Follow Up, frontal and sagittal views


Published with the approval of Dr. Ali Maziad